


 Sign Out
Sign Out

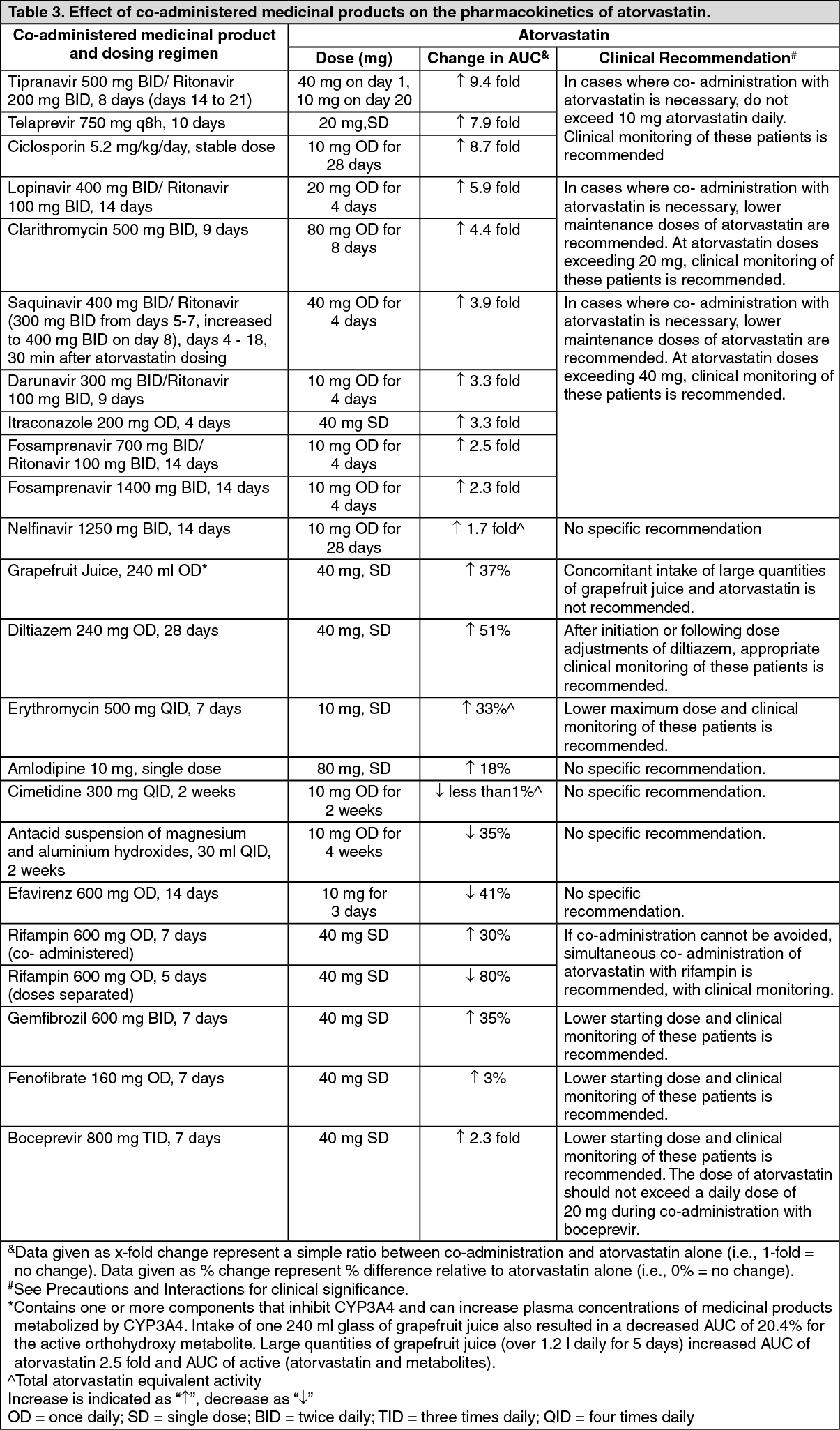
CYP3A4 inhibitors: Potent CYP3A4 inhibitors have been shown to lead to markedly increased concentrations of atorvastatin (see Table 3 and specific information as follows). Co-administration of potent CYP3A4 inhibitors (e.g. ciclosporin, telithromycin, clarithromycin, delavirdine, stiripentol, ketoconazole, voriconazole, itraconazole, posaconazole and HIV protease inhibitors including ritonavir, lopinavir, atazanavir, indinavir, darunavir, etc.) should be avoided if possible. In cases where co-administration of these medicinal products with atorvastatin cannot be avoided lower starting and maximum doses of atorvastatin should be considered and appropriate clinical monitoring of the patient is recommended (see Table 3).
Moderate CYP3A4 inhibitors (e.g. erythromycin, diltiazem, verapamil and fluconazole) may increase plasma concentrations of atorvastatin (see Table 3). An increased risk of myopathy has been observed with the use of erythromycin in combination with statins. Interaction studies evaluating the effects of amiodarone or verapamil on atorvastatin have not been conducted. Both amiodarone and verapamil are known to inhibit CYP3A4 activity and coadministration with atorvastatin may result in increased exposure to atorvastatin. Therefore, a lower maximum dose of atorvastatin should be considered and appropriate clinical monitoring of the patient is recommended when concomitantly used with moderate CYP3A4 inhibitors. Appropriate clinical monitoring is recommended after initiation or following dose adjustments of the inhibitor.
CYP3A4 inducers: Concomitant administration of atorvastatin with inducers of cytochrome P450 3A (e.g. efavirenz, rifampin, St. John's Wort) can lead to variable reductions in plasma concentrations of atorvastatin. Due to the dual interaction mechanism of rifampin, (cytochrome P450 3A induction and inhibition of hepatocyte uptake transporter OATP1B1), simultaneous coadministration of atorvastatin with rifampin is recommended, as delayed administration of atorvastatin after administration of rifampin has been associated with a significant reduction in atorvastatin plasma concentrations. The effect of rifampin on atorvastatin concentrations in hepatocytes is, however, unknown and if concomitant administration cannot be avoided, patients should be carefully monitored for efficacy.
Transport protein inhibitors: Inhibitors of transport proteins (e.g. ciclosporin) can increase the systemic exposure of atorvastatin (see Table 3). The effect of inhibition of hepatic uptake transporters on atorvastatin concentrations in hepatocytes is unknown. If concomitant administration cannot be avoided, a dose reduction and clinical monitoring for efficacy is recommended (see Table 3).
Gemfibrozil/fibric acid derivatives: The use of fibrates alone is occasionally associated with muscle related events, including rhabdomyolysis. The risk of these events may be increased with the concomitant use of fibric acid derivatives and atorvastatin. If concomitant administration cannot be avoided, the lowest dose of atorvastatin to achieve the therapeutic objective should be used and the patients should be appropriately monitored (see Precautions).
Ezetimibe: The use of ezetimibe alone is associated with muscle related events, including rhabdomyolysis. The risk of these events may therefore be increased with concomitant use of ezetimibe and atorvastatin. Appropriate clinical monitoring of these patients is recommended.
Colestipol: Plasma concentrations of atorvastatin and its active metabolites were lower (by approx. 25%) when colestipol was coadministered with atorvastatin. However, lipid effects were greater when atorvastatin and colestipol were co-administered than when either medicinal product was given alone.
Fusidic acid: Interaction studies with atorvastatin and fusidic acid have not been conducted. As with other statins, muscle related events, including rhabdomyolysis, have been reported in postmarketing experience with atorvastatin and fusidic acid given concurrently. The mechanism of this interaction is not known. Patients should be closely monitored and temporary suspension of atorvastatin treatment may be appropriate.
Colchicine: Although interaction studies with atorvastatin and colchicine have not been conducted, cases of myopathy have been reported with atorvastatin co-administered with colchicine, and caution should be exercised when prescribing atorvastatin with colchicine.
Effect of atorvastatin on co-administered medicinal products: Digoxin: When multiple doses of digoxin and 10 mg atorvastatin were co-administered, steady-state digoxin concentrations increased slightly. Patients taking digoxin should be monitored appropriately.
Oral contraceptives: Co-administration of atorvastatin with an oral contraceptive produced increases in plasma concentrations of norethindrone and ethinyl oestradiol.
Warfarin: In a clinical study in patients receiving chronic warfarin therapy, coadministration of atorvastatin 80 mg daily with warfarin caused a small decrease of about 1.7 seconds in prothrombin time during the first 4 days of dosing which returned to normal within 15 days of atorvastatin treatment. Although only very rare cases of clinically significant anticoagulant interactions have been reported, prothrombin time should be determined before starting atorvastatin in patients taking coumarin anticoagulants and frequently enough during early therapy to ensure that no significant alteration of prothrombin time occurs. Once a stable prothrombin time has been documented, prothrombin times can be monitored at the intervals usually recommended for patients on coumarin anticoagulants. If the dose of atorvastatin is changed or discontinued, the same procedure should be repeated. Atorvastatin therapy has not been associated with bleeding or with changes in prothrombin time in patients not taking anticoagulants.
Paediatric population: Drug-drug interaction studies have only been performed in adults. The extent of interactions in the paediatric population is not known. The above mentioned interactions for adults and the warnings in Precautions should be taken into account for the paediatric population. (See Tables 3 & 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image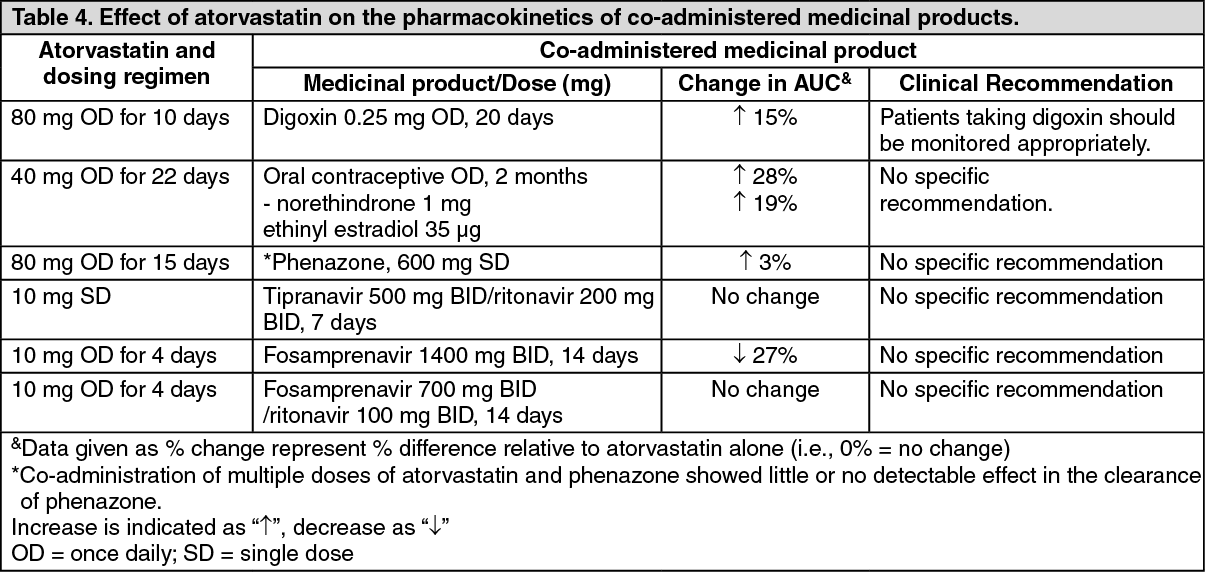 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image